
Continuous cystine control is critical to limiting the progression of cystinosis. Even a brief interruption in cysteamine administration can result in a rapid return to toxic levels of cystine.1
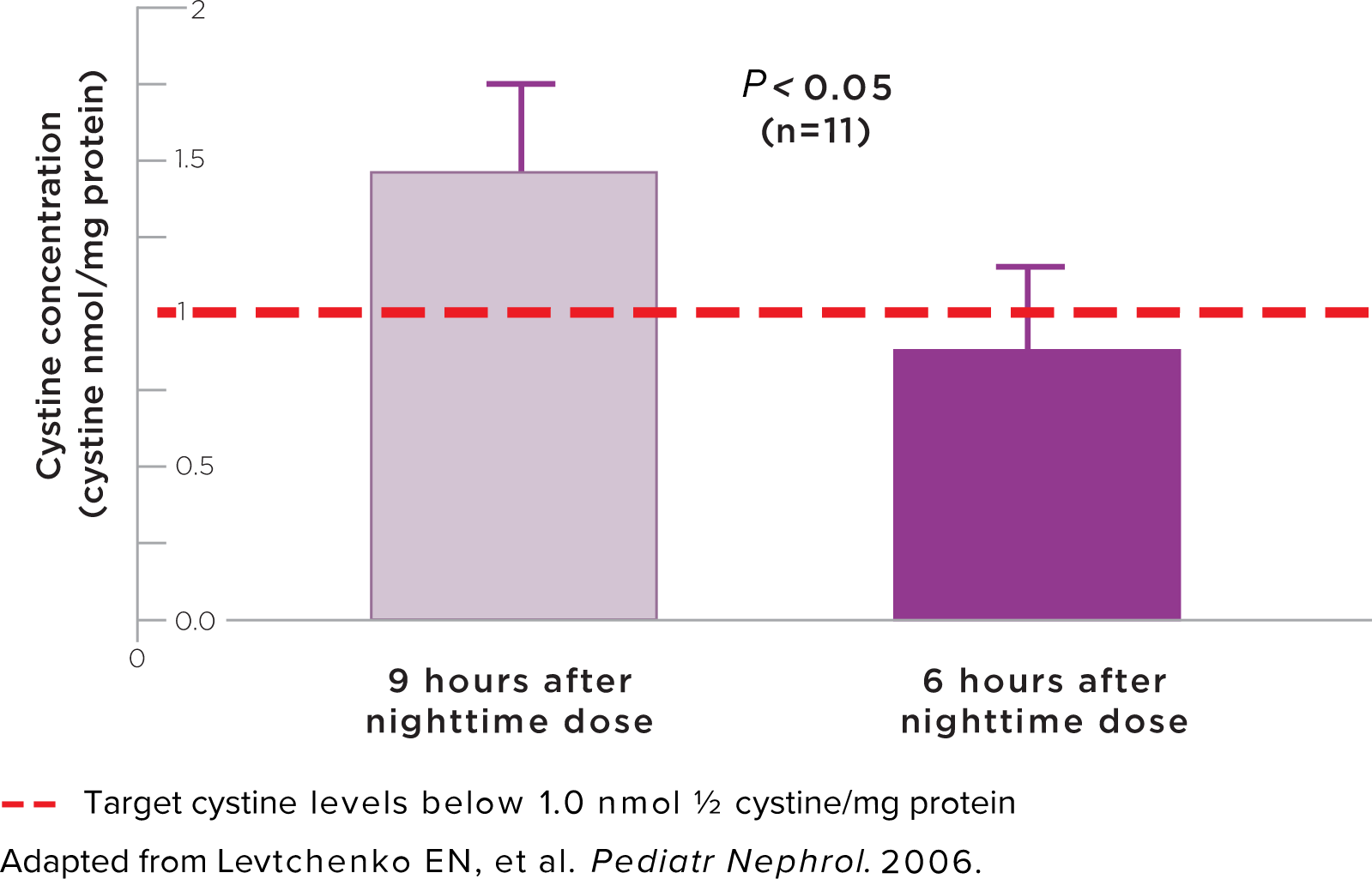
In a study, when patients had a longer interval between their dose of cystine-depleting therapy (CDT) by 3 hours (9 hours vs 6 hours) they had white blood cell (WBC) cystine levels that were 65% higher than when they had a shorter timeframe.1
Comparison of WBC cystine content with immediate-release (IR) cysteamine
administered at 9 hours vs 6 hours after nighttime dose1
Comparison of morning leukocyte content with IR CDT when administered every 6 hours (8 AM, 2 PM, 8 PM, 2 AM) vs 4 times a day with a 9-hour night pause (8 AM, 1 PM, 6 PM, 11 PM) in a cohort of 22 Dutch patients (mean age 14.7 ± 9.7 years) with nephropathic cystinosis.5
WBC cystine levels should be regularly measured to help ensure optimal PROCYSBI dosing2
The PROCYSBI maintenance dose should be individualized based on therapeutic goals and WBC cystine levels. For patients who have achieved the target therapeutic WBC cystine level, monitor WBC cystine concentration at least twice a year.2
Monitoring Frequency2
-
2 weeks after PROCYSBI initiation
-
Once therapeutic target is achieved, monitor quarterly for 6 months
-
Then twice yearly (at minimum)
-
2 weeks after PROCYSBI initiation
-
Then monitor until the target WBC cystine concentration is achieved
-
Then monthly for 3 months
-
Then quarterly for 1 year
-
Then twice yearly (at minimum)
-
Obtain measurement after reaching the maintenance PROCYSBI dosage
-
Then monthly for 3 months
-
Then quarterly for 1 year
-
Then twice yearly (at minimum)
Maintenance doses may require adjustment to achieve the target WBC cystine levels.2
If the WBC cystine concentration is greater than the target level, consider the following before dose adjustment2:
-
Adherence to medication and dosing interval
-
The timing between the last dose and the blood draw for the laboratory measurement
-
The timing of PROCYSBI administration in relation to food or other administration instructions
Regular WBC cystine level testing is an important element in the effective treatment of cystinosis2-4
Two WBC cystine level tests are available but cannot be used interchangeably.4,5 The same type of test should be used consistently to achieve comparable results. Instruct patients to get a trough blood test and to take PROCYSBI immediately after. It’s recommended to use the same test type each time in order to compare results over time.2 Be sure to recommend that your patients obtain their blood draw just before they take their next dose of PROCYSBI.2,4
|
Type of Test |
Testing Institution |
Test-Specific Target Cystine Level5 |
|---|---|---|
|
Granulocytes |
University of California San Diego |
Less than 1.9 nmol ½ cystine/mg protein |
|
Mixed leukocytes |
Baylor Genetics |
Less than 1.0 nmol ½ cystine/mg protein |
Timing of WBC Monitoring2
Obtain WBC sample 12 hours after dosing with PROCYSBI. It is important to accurately record the time of the last dose, the actual dose, and the time the blood sample was taken.

Have more questions?

Find Out More About the Benefits of PROCYSBI
Review helpful resources and tools for you and your patients.
1. Levtchenko EN, van Dael CM, de Graaf-Hess AC, et al. Strict cysteamine dose regimen is required to prevent nocturnal cystine accumulation in cystinosis. Pediatr Nephrol. 2006;21(1):110-113. 2. PROCYSBI (cysteamine bitartrate) delayed-release capsules and delayed-release oral granules [prescribing information] Amgen. 3. Elmonem MA, Veys KR, Soliman NA, van Dyck M, van den Heuvel LP, Levtchenko E. Cystinosis: a review. Orphanet J Rare Dis. 2016;11(47):1-17. 4. Langman CB, Barshop BA, Deschênes G, et al. Controversies and research agenda in nephropathic cystinosis: conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2016;89(6):1192-1203. 5. Gertsman I, Johnson WS, Nishikawa C, Gangoiti JA, Holmes B, Barshop BA. Diagnosis and monitoring of cystinosis using immunomagnetically purified granulocytes. Clin Chem. 2016;62(5):766-772.